
Practice Perfect 959
No More Opioids for Postoperative Pain?
No More Opioids for Postoperative Pain?


The holy grail for postoperative pain management in all surgery is the elimination of the need for opioids. This is no less true for foot and ankle surgery. We’re all aware of the opioid crisis, and everyone is becoming hypersensitive to prescribing medications with a high addiction and abuse potential. We also know that foot and ankle surgery is not a pain-free endeavor. Thus, the need for an opioid-free, effective postoperative protocol would be very helpful and much welcomed.
Enter a new randomized controlled trial recently published in the Journal of Bone and Joint Surgery by Turk and colleagues1 that provides a hopeful view on the topic. This study has some complexity in design and execution, so I’ll direct the interested reader to the study itself for a more detailed read. For today, we’ll cover the main details for your consideration.
As an overall summary, this research group, based out of North Carolina, randomized patients undergoing a number of different orthopedic procedures (including foot and ankle procedures) to a pain management protocol that either included or excluded an opioid medication. The study was not blinded. A summary of the two pain management arms for the foot and ankle surgery group is shown in Table 1. This study focused on surgical procedures for bunions and hallux rigidus. Unfortunately, this did not include hindfoot or ankle procedures.
Table 1. Experimental Pain Management Protocols for Nonopioid and Opioid Use
| Nonopioid Pathway (157 total patients) | Opioid Pathway (158 total patients) |
Preoperative:
|
Preoperative:
|
Intraoperative:
|
Intraoperative:
|
PACU:
|
PACU:
|
Discharge:
|
Discharge:
|




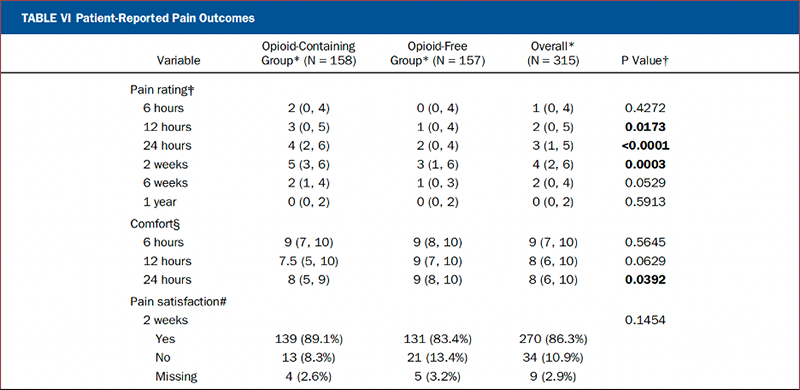
The primary outcome was the numeric pain scale (0-10) at 24 hours. The secondary outcome was patient-perceived “comfort” which included pain, nausea, vomiting, and constipation. The secondary outcomes were surveyed at 6 and 12 hours postop and at 2 and 6 weeks postop, and at 1 year. They tracked a number of other outcomes, but we’ll omit those for the sake of our current discussion.
The study indicates the nonopioid pain management regimen to be noninferior to the opioid method and was superior at pain control at the 6-hr, 12-hr, and 2-week time periods.
The results of the study indicate the nonopioid pain management regimen to be noninferior to the opioid method and was superior at pain control at the 6-hr, 12-hr, and 2-week time periods. They also reported improved patient comfort at 12 and 24-hours (likely due to the decreased nausea, vomiting, and constipation seen with opioids) and superior patient satisfaction with pain at 6-weeks. I included a portion of the study’s Table VI to show their primary outcome results. Overall, 29 patients in the opioid-free group required opioids for breakthrough pain (but this was reported for the entire multi-specialty group and not isolated to the foot and ankle group).
I read this as very hopeful news, but there are several issues for us foot and ankle surgeons to consider. First, I’d love to see a study like this repeated for only foot and ankle procedures to improve the generalizability of the study.
Second, although the demographics were stated to be nonsignificant (theoretically eliminating this as a factor), there were a lot more females than males in the study. In my experience, females generally handle pain better than males, so this may have skewed the results somewhat. However, the numbers in the groups were equivalent, so we’ll give the authors a break on this one.
Third, as you can see from our first table, the non-opioid pathway was medication heavy (as one might imagine), and the opioid pathway was very light. In reality, many surgeons still combine therapies. For example, if I perform an ankle arthrodesis, I will include a popliteal and adductor canal block preoperatively along with postoperative opioids. We should think about the limited options used in the opioid group as maintaining a clean, easier to analyze control group rather than as a “standard of care” interpretation. In fact, one might question which medications in the multi-modality non-opioid group had the greatest effect on the primary outcome? I’m going to completely avoid the discussion of cost here, which is also a valid question. IV acetaminophen isn’t cheap.
For me, the outcomes are encouraging, but they don’t eliminate opioid need just yet. This study adds to the mounting body of evidence that a multi-modality approach to perioperative pain management is reasonable, legitimate, and evidence based. When added to concepts such as the ERAS (enhanced recovery after surgery) protocols (see Practice Perfect 659 - The New Enhanced Recovery After Surgery Protocol Part 1: What is it? and Practice Perfect 660 - ERAS Protocol Part 2: What’s the Evidence?), it seems relatively clear that an approach such as that advocated by the authors of this study has the potential to significantly decrease the use of opioids for most patients.
Best wishes.

Jarrod Shapiro, DPM
PRESENT Practice Perfect Editor
[email protected]

- Turk R, Averkamp B, Hietpas K, Michalek C, Leas D, Odum SM, Hamid N. CORE Study Group. An Opioid-Free Perioperative Pain Protocol Is Noninferior to Opioid-Containing Management: A Randomized Controlled Trial. J Bone Joint Surg Am. 2025 Apr 2:107:665-677.
Follow this link
This ezine and the overall sponsorship of PRESENT Podiatry was made possible through the support of our sponsors:
















Comments
There are 0 comments for this article